7 June 2026
How to build a competitive portfolio for SEM ST3 training
If you are serious about applying for sport and exercise medicine (SEM) higher specialty training in the UK, the portfolio is where it starts. Not at the interview. Not on the day you submit your Oriel application. It starts months or years earlier, with the decisions you make about where to spend your time and energy during core training.
This article breaks down exactly how the SEM ST3 application is scored, what you need to achieve maximum marks in each domain, and practical strategies for getting there efficiently. It is written for doctors currently in or approaching Internal Medicine Training (IMT), GP Specialty Training (GPST), or Acute Care Common Stem (ACCS) who plan to apply for SEM at ST3. If you are not sure which of those routes to take, I covered the comparison in detail in How to become a sport and exercise medicine doctor in the UK.
A note before we start. The scoring criteria described here are based on the current framework published by Physician Higher Specialty Training (PHST) recruitment at the time of writing. These criteria can and do change between recruitment rounds. Before you plan anything, go to the PHST website, navigate to Sport & Exercise Medicine, and check the current self-assessment scoring framework under the 'Planning your application' tab. You can also access the scoring page directly here. What I am describing below is the structure as it stands now. Use it as a guide, not a guarantee.
How competitive is it?
The numbers tell the story. In the 2025 recruitment round, 107 doctors applied for 12 SEM training posts nationally. That is a competition ratio of 8.9 to 1. For context, in 2018 it was 2.7 to 1. In 2022, it hit 9.0 to 1 with only 5 posts. The trajectory is clear and it is likely to keep rising as more doctors become aware of the specialty.
This is not a specialty where you can coast on a decent CV and hope for the best. The candidates who succeed are the ones who understand the scoring framework, plan strategically, and build their portfolios with purpose.
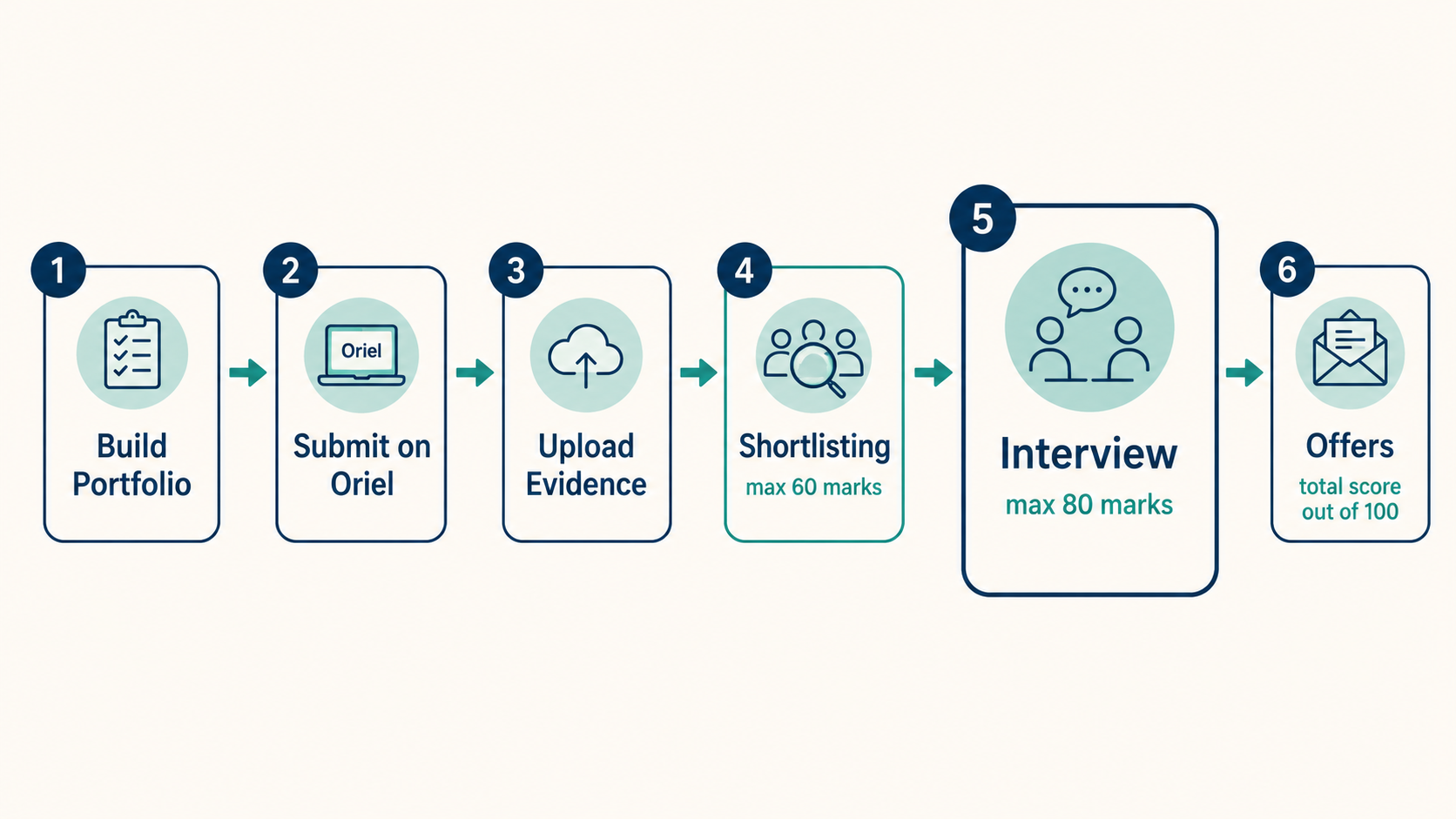
How the application works
Applications are submitted through the Oriel platform. The application form includes a self-assessment section where you score yourself across multiple domains based on your achievements. There are 38 points available across the self-assessment domains, plus 2 additional marks for how well you organise and present your evidence documents. That gives a maximum application score of 40.
After you submit, you will be asked to upload evidence to support your self-assessment scores. Assessors will verify your claims against the evidence you provide. If your evidence is unclear or insufficient, your score can be adjusted downward. If you gain an achievement between submission and the evidence upload deadline, you are permitted to include it and can be scored accordingly.
Your verified application score is used for shortlisting. If you are shortlisted, you progress to interview. At interview, your application score is weighted by 0.5 (so the maximum 40 becomes 20 out of 100), while the interview itself carries up to 80 marks. The portfolio gets you into the room. The interview is what determines the offer. Both matter.
The scoring domains
The application is scored across eight domains. Here is a summary of each and the maximum marks available. The rest of this article will go through them one by one, focusing on what you need for top marks.
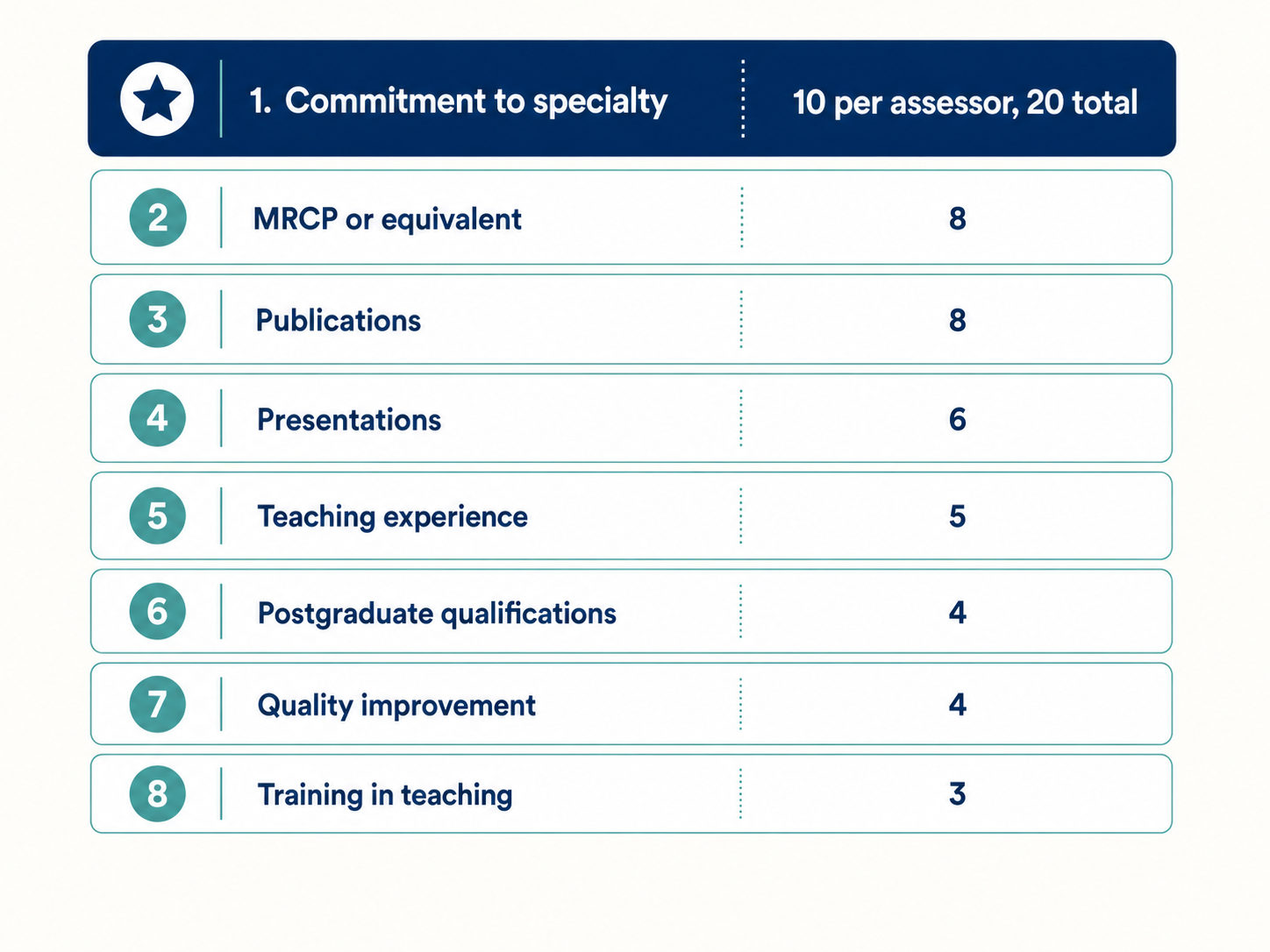
Commitment to specialty is scored separately by two independent assessors rather than through self-assessment. The remaining seven domains make up the 38-point self-assessment total. There are also two further marks for the organisation and quality of your evidence documents, which I will cover separately at the end.
Commitment to specialty: 10 points per assessor (20 total)
This is the single largest component of the shortlisting score. Two independent assessors will each award you between 0 and 10 points based on their review of your application, giving a combined maximum of 20 marks. That makes commitment 20 out of 60 possible shortlisting marks, or a third of the total.
For SEM, commitment is also assessed at interview, where the suitability and commitment station is weighted at 2.5, making it worth up to 25 out of 80 interview marks. So commitment is tested twice: once at shortlisting and again at interview. It is the thread that runs through everything.
To score 10 out of 10 from each assessor, you need to demonstrate a good level of commitment to the specialty, undertaking a range of activities or experiences commensurate with your stage of training, and a good understanding of the skills and attributes required.
What does that look like in practice? Go to conferences, talks, and educational events relevant to SEM and collect certificates. Organise electives, shadowing, internships, or placements that give you direct exposure to sports medicine practice. Volunteer at sporting events such as the London Marathon, parkruns, or local club fixtures. Get involved in projects related to sports medicine, whether that is research, audit, or clinical work. Show genuine, sustained interest and demonstrate that you have actively sought opportunities rather than passively waited for them.
The assessors are aware that candidates at different stages of training will have had different opportunities. You are not expected to have covered pitchside at the Premier League during your F2 year. But you are expected to have done something deliberate and consistent. Particular credit is given to activities that did not require a financial outlay or did not arise as part of your clinical placements, because these show initiative.
The scoring anchor at the bottom end is worth knowing: a score of 0 means no or very little demonstration of commitment, where the candidate is unable to express meaningful engagement with the specialty and any references to interest are subjective with no supporting examples. A candidate marked as not appointable by either assessor will not be shortlisted, regardless of their self-assessment score.
Build your commitment evidence from day one. Every conference certificate, every letter from a supervisor, every volunteering placement you document now is a piece of evidence you will not need to reconstruct later.
MRCP(UK) or equivalent: 8 points
This is tied as the highest-scoring self-assessment domain and for most applicants the most straightforward. You get 8 points for passing both MRCP(UK) Part 2 Written and PACES, which requires having already passed Part 1.
If you are coming through the IMT route, this means completing your full MRCP. If you trained through GPST, you score the equivalent 8 points for holding full MRCGP. Through ACCS, the equivalent is full MRCEM. The person specification lists the accepted alternatives, and you should check it directly, but the principle is the same across all three training pathways: complete your exit exam.
This is not a domain where strategy comes in. It is a domain where you simply need to pass. If you have not done so by the time you apply, you lose 8 points against candidates who have. That is a significant gap to make up elsewhere.
Publications: 8 points
To score maximum marks you need to be first author, joint-first author, or corresponding author of one or more PubMed-cited original research publications. The publication can be in press (fully accepted, awaiting publication) at the time of application.
The key detail here is what counts as original research. Systematic reviews count. This is the route most applicants take, and for good reason. A systematic review is something you can initiate, lead, and drive to publication without needing access to a lab, a patient cohort, or ethics approval for a clinical trial. It is the most accessible form of original research available to a trainee working full-time clinical shifts.
My advice is to aim for a systematic review without a meta-analysis if your priority is speed and feasibility. A meta-analysis adds statistical complexity and delays without changing your score. Pick a clinically meaningful question within SEM, follow the PRISMA guidelines, register your protocol on PROSPERO, do the work, and submit to a PubMed-indexed journal. If you are first or joint-first author, you score 8 points.
Co-authorship on original research scores 6 points. Being first author of a non-original piece (case report, editorial, review) scores less. Aim for first-author original research. It is the gold standard for this domain and the difference between 8 and 5 or 6 points adds up.
Presentations: 6 points
Maximum marks require an oral presentation at a national or international medical meeting where you were first or second author. An important clarification: you do not need to have personally delivered the presentation to score these points. What matters is that you are listed as first or second author on the presentation and that the meeting qualifies as national or international.
National meetings must be open to anyone in the country. International meetings must be open to attendees from a range of countries. For scoring purposes, the home UK nations are treated as separate nations. A presentation at a Scotland-wide medical meeting counts as national.
You need evidence that your presentation was accepted and included at the meeting. This means a confirmatory letter, certificate, or evidence of inclusion in the abstracts book. National and international claims that are not accompanied by a document listing the accepted abstracts may be downgraded during evidence verification.
Here is the efficiency tip. If you have published a systematic review (see above), submit the same study as an oral presentation abstract to a national or international conference. Many conferences in the SEM space accept abstract submissions with a fee. Apply, pay the fee, present your work, and collect your certificate. One piece of research, two high-scoring portfolio items. If you can present at a conference relevant to SEM, such as a BASEM or FSEM event, that also strengthens your commitment narrative.
A poster at a national or international meeting scores 4 points, and an oral presentation at a regional meeting scores 3. Both are worth having, but aim for the oral at national or international level if you can.
Teaching experience: 5 points
The top score requires that you have worked with local tutors to organise a teaching programme (a series of sessions) for healthcare professionals or medical students, taught regularly on that programme over approximately three months or longer, and have evidence of formal feedback.
The wording is important. You need to have worked with local tutors to organise the programme and arrange teachers. You do not need to have personally designed the entire programme. But you do need a certificate or letter of recognition confirming your contribution, and evidence of formal feedback from the sessions. Formal feedback means either collected participant feedback forms with a summary, or a completed Developing the Clinical Teacher or Teaching Observation form.
If you are on a GP rotation, this fits naturally. Many GP trainees are expected to organise or contribute to teaching programmes as part of their training requirements. Use that overlap. Set up a teaching series for medical students or junior colleagues at your practice over a few months, arrange speakers, collect formal feedback using a simple Google Form, and ask your supervisor for a letter confirming your role. The work you would be doing anyway becomes a portfolio item.
If you are not in GP training, look for opportunities wherever you are. Teaching programmes can run in any clinical setting. Three months of regular sessions with documented feedback is the target.
Postgraduate qualifications: 4 points
A PhD or MD by research scores the maximum 4 points. However, most applicants will realistically be aiming at the next tier: 3 points for a masters-level degree (MSc, MA, MRes) of at least eight months' duration full-time equivalent.
My strong recommendation is to choose an MSc in Sport and Exercise Medicine specifically. The reason goes beyond the portfolio score. Many sports medicine jobs, both during and after training, list an MSc in SEM or a related field as an essential or desirable criterion. Getting the MSc now serves you twice: once for your ST3 application, and again every time you apply for a clinical post or an extended role for the rest of your career.
Intercalated degrees cannot be scored in this section, regardless of the level at which they were awarded. Postgraduate teaching qualifications (PG Cert, PG Dip in teaching) should not be scored here either, as they belong in the separate Training in Teaching domain.
Quality improvement: 4 points
Maximum marks require involvement in all aspects of two cycles of a quality improvement project where you can demonstrate a leadership role, including designing the project, playing a leading role in delivery, and supervising other team members. The project must use recognised QI methodology such as Plan-Do-Study-Act (PDSA) cycles.
The key distinction between 4 and 3 points is leadership. Involvement in all aspects of two cycles without a demonstrable leadership role scores 3. To get 4, you need evidence that you designed the project, led its delivery, and supervised others. Your evidence should include a completed QIPAT form or equivalent headed letter from your supervisor confirming the topic, methodology, your role, the results, and what was learned.
As with teaching, if you are on a GP rotation, QI projects often fit naturally into the training requirements. Run your QI project there if you can. Choose a topic relevant to SEM or musculoskeletal care if possible, because while the project does not need to be SEM-related for scoring purposes, having an SEM-relevant project strengthens your commitment narrative at interview.
Training in teaching: 3 points
A postgraduate qualification in teaching at PG Certificate or PG Diploma level scores the full 3 points. The qualification must be a university-accredited programme worth at least 60 credit points, open only to graduate entrants.
If you have a genuine interest in medical education, there are excellent options. I did the PG Certificate in Clinical Education at King's College London. It was intensive, with weekly in-person classes, substantial assignments, and a significant reading commitment. But I learned a great deal and came out with Fellowship of the Higher Education Academy (FHEA), which is useful for anyone interested in teaching roles beyond clinical practice.
If your interest is primarily in scoring the points, the most pragmatic approach is to find the cheapest accredited online PG Certificate in teaching you can, complete it, and move on. The score does not differentiate between programmes. Three points is three points whether it came from a prestigious in-person course or an affordable distance-learning option.
Training below PG Certificate level (for example, a one-day teaching skills course of at least six hours) scores 1 point.
Evidence: the 2 marks that feel small but are not
There are 2 additional marks available for how well you organise and present your evidence documents. That sounds minor. It is not. The PHST guidance states explicitly that if the presentation of your evidence is sufficiently poor, it could lead to your application not being shortlisted regardless of your other scores.
Evidence must be clear, well-organised, and easy for assessors to verify quickly. Each scoring domain that requires evidence has a pro forma available in the PHST document library that must be completed and uploaded. Beyond the pro formas, keep it clean. A logical folder structure, clearly labelled documents, relevant certificates and letters front and centre. Do not bury assessors in excessive documentation, but make sure everything they need is there.
Along the way, collect proof of everything. Certificates for conferences and courses. Letters from consultants confirming your involvement in projects. Teaching feedback collected on paper or through Google Forms. QIPAT forms signed by supervisors. PubMed screenshots with your name visible. The candidates who score best are the ones who have been gathering evidence systematically throughout their training, not scrambling to reconstruct it the week before the upload deadline.
Practical tips for building your portfolio
These are the things I would tell someone sitting down to plan their SEM application with 12 to 18 months to go.
Start with one piece of research and make it count twice. Publish a systematic review as first author (8 points for publications), then present the same work as an oral presentation at a national or international conference (6 points for presentations). That is 14 points from a single project.
Choose an MSc in Sport and Exercise Medicine specifically. You get 3 points for the postgraduate qualification domain, and you get a credential that many SEM and MSK job adverts list as essential or desirable. That investment pays for itself long after the application.
Use your GP rotation strategically. If you are on the GPST route, GP placements typically offer more predictable hours and more flexibility to set up teaching programmes, QI projects, and additional activities. Many GP training programmes already require you to do teaching and QI, so align those requirements with your SEM portfolio. Two birds, one stone.
Embed portfolio activities into your NHS commitments wherever possible. Running a QI project? Pick an MSK or physical-activity topic in your current department. Organising a teaching programme? Make it relevant to sports medicine or MSK assessment. Everything counts more when it reinforces the same narrative.
Get your teaching qualification done early. It is a fixed number of points for completing a course. There is no advantage to leaving it late. If it is purely for the score, find an affordable online PG Certificate, do it alongside your clinical work, and bank the 3 points.
Remember that achievements do not need to be SEM-related to score points in the self-assessment, but SEM-related achievements are stronger for two reasons: they contribute to your commitment score at shortlisting and at interview, and they demonstrate genuine insight into the specialty you are applying to. A QI project on clinic waiting times in an MSK service tells a more compelling story than one on ward handovers, even if the self-assessment score is identical.
The scoring criteria can change
I want to end on this because it is the most important caveat. The self-assessment framework, the domain weightings, and the scoring criteria are reviewed and updated by PHST. They can change between recruitment rounds. Everything in this article reflects the framework at the time of writing. Before you finalise your plans, check the current person specification on the PHST website and the self-assessment scoring framework. Navigate to the Sport & Exercise Medicine specialty page and read the guidance under 'Planning your application'. If something has changed since this article was published, the PHST website is the authority, not this page.
Building a competitive SEM portfolio takes sustained effort over months and years. But there is nothing mysterious about it. The scoring framework is published. The criteria are explicit. The top-scoring candidates are not the ones with the most raw talent. They are the ones who understood the system earliest, planned their time deliberately, and collected the evidence to prove it.