17 May 2026
How to become a sport and exercise medicine doctor in the UK
What sport and exercise medicine actually is
Sport and exercise medicine (SEM) is a medical specialty. That distinction matters because most people outside the field assume it is either a branch of orthopaedic surgery or a vague label for doctors who happen to work with athletes. It is neither.
SEM is one of the newest medical specialties in the UK, formally recognised by the GMC in 2005 in the run-up to the London 2012 Olympics. It is a Group 2 specialty, which means it requires prior core training before entry. The specialty sits within medicine, not surgery. SEM doctors do not operate. The procedural side of SEM is usually limited to areas such as injection therapy and ultrasound-guided procedures. Some clinicians may also work with treatments such as PRP or spinal interventional procedures in specific, appropriately governed settings, but these are not universal parts of SEM practice. If you want to do ACL reconstructions and arthroscopies, that is sports surgery, which is a subspecialty interest developed through orthopaedic training and post-CCT fellowships. Different career, different pathway.
What SEM doctors actually do is broader than most people expect. The core involves treating musculoskeletal injuries and conditions, using exercise as a treatment for chronic disease, preventing illness through physical activity, and providing medical care in sporting environments with the clinical nuances that come with managing athletes. Within that, there are several interest areas and portfolio niches you can develop:
- Musculoskeletal medicine
- Team and pitchside sports medicine
- Sports cardiology
- Dance, performance, and artistic sports medicine
- Paediatric sports medicine
- Women's health in SEM
- Military and occupational SEM
- Sports rheumatology
- Ultrasound and imaging-focused SEM
- Sports neurology
- Public health and physical activity promotion
You can work with essentially any sport. Football doctor, tennis doctor, Formula 1 doctor, dive doctor, golf doctor, ringside doctor. The settings are equally varied: NHS MSK clinics, ultrasound and injection clinics, professional clubs and national teams, Ministry of Defence rehabilitation hospitals, private clinics, public health organisations, and national and international sports bodies. SEM consultant careers are often portfolio-based, combining several of these settings rather than sitting in a single role.
Two organisations have historically shaped the UK SEM landscape. The Faculty of Sport and Exercise Medicine UK (FSEM) is the professional body responsible for training, examinations, standards, and specialty representation. The British Association of Sport and Exercise Medicine (BASEM) is the major membership organisation focused on education, events, networking, and advocacy. At the time of writing, FSEM and BASEM are progressing towards forming the College of Sport, Exercise and Musculoskeletal Medicine (CSEM). Both organisations continue to operate separately until the reformation is formally completed, so by the time you read this the naming and structure may have changed.
The formal training pathway
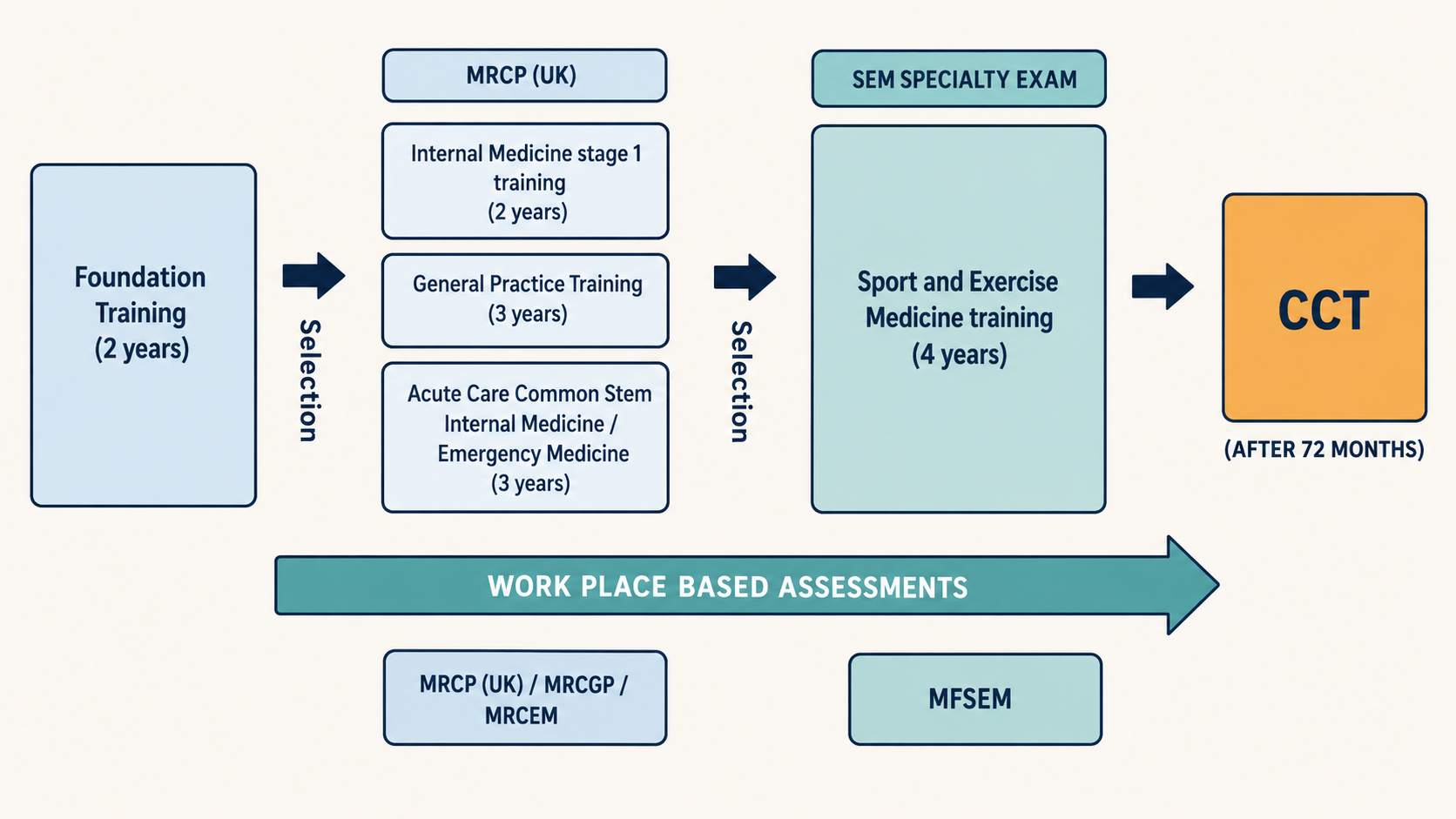
The standard route to becoming an SEM consultant runs through higher specialty training (HST), which for SEM spans ST3 to ST6. Four years, starting after you have completed foundation training and a recognised core training programme.
Here is the sequence in full. You graduate from medical school, complete the two-year foundation programme (F1 and F2), then enter one of three core training pathways that qualify you to apply for SEM at ST3. Once accepted, you train for four years, achieve your Certificate of Completion of Training (CCT) at the end of ST6, and become an SEM consultant.
The three core training routes that qualify you are:
- Internal Medicine Training (IMT): completion of Internal Medicine stage 1 with the required MRCP milestones, generally after two years
- Acute Care Common Stem (ACCS): usually three years, providing an acute-care route into SEM. The specific exam requirements (MRCEM or FRCEM Intermediate Certificate for emergency medicine applicants, or MRCP milestones for ACCS-IM applicants) depend on which ACCS stream you follow
- GP Specialty Training (GPST): three years, leading to MRCGP and GP Register eligibility
Any of these three will make you eligible to apply for SEM ST3. You only need one. I will compare them in the next section. Recruitment rules, exam requirements, and membership pathways can and do change, so always check the current person specification on the FSEM and national recruitment pages before applying.
How competitive is it? The 2025 application round had 12 training posts nationally, including a recently added post in Scotland. There were 107 applicants, giving a competition ratio of 8.92. That ratio has sat high in recent years. It may rise further if awareness of the specialty continues to grow faster than training-post expansion, but competition ratios should be treated as a broad guide rather than a prediction.
Once you complete ST6 and receive your CCT, you are a consultant in sport and exercise medicine. You can then work in any of the settings I described above, or combine several of them.
Comparing the three core training routes
This is the decision that shapes the first few years of your career in medicine, and it has real consequences for your route into SEM. All three qualify you equally for ST3 applications, but they give you very different skills, timelines, and options.
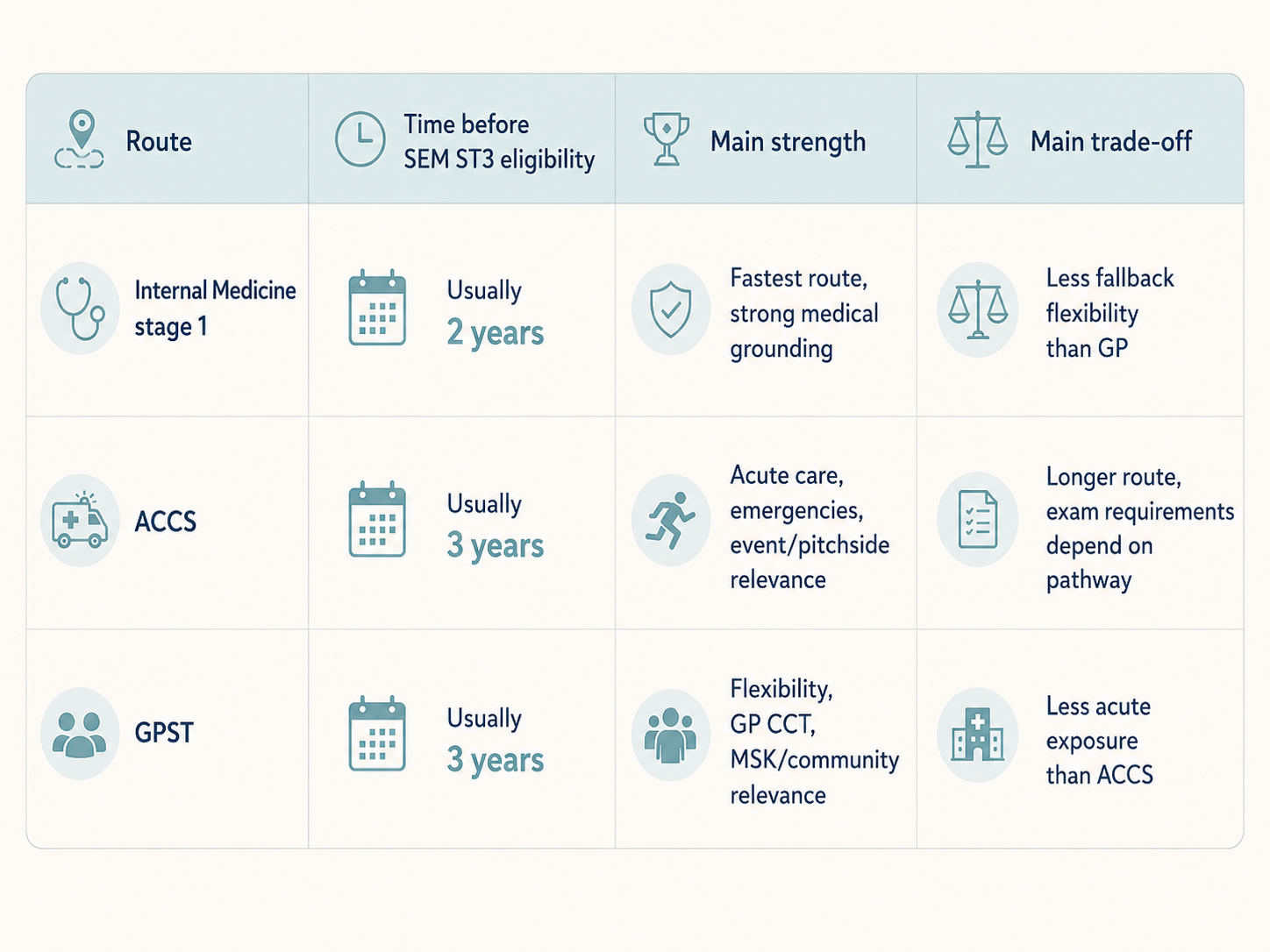
Internal Medicine Training
Two years to complete Internal Medicine stage 1. This is the fastest route to SEM eligibility. You come out with MRCP and a broad grounding in general internal medicine, which is more relevant to SEM than people sometimes realise. A lot of SEM practice involves managing medical conditions in athletes (cardiac screening, diabetes, respiratory problems during exercise, complex medication decisions for active patients), and IMT gives you the clinical confidence to handle that end of the specialty.
The downside is that IMT does not give you a standalone CCT or GP Register eligibility. If you decide halfway through SEM training that it is not for you, your fallback position is less clear than it would be with GP training behind you.
ACCS
Usually three years. This is the route to choose if your interest in SEM leans towards the acute end: pitchside medicine, motorsport, rugby, combat sports, event medical cover, or any setting where you are the first responder when something goes wrong. ACCS gives you hands-on procedural skills, experience managing acutely unwell patients under pressure, and the clinical confidence to work in high-stakes, time-critical environments.
The extra year compared to IMT is the trade-off. Three years of core training before you even start SEM specialty training means a longer total journey to consultant level. But if your eventual SEM practice will involve standing pitchside or trackside making rapid clinical decisions, ACCS gives you the strongest foundation for that work.
GP Specialty Training
Three years. This is, in my view, the most strategically flexible of the three, for reasons that go beyond the training itself.
First, GPST gives you a CCT in General Practice and entry onto the GP Register. If you later complete SEM training as well, you would hold both a GP CCT and an SEM CCT, with the associated registration routes. That is a strong position to be in professionally.
Second, GP training typically involves fewer on-call commitments than IMT or ACCS, which means you have more time in the evenings and weekends to build a portfolio in sport and exercise medicine. You can work with local sports teams, provide medical cover at events, take FSEM diplomas, and develop the CV that makes your ST3 application competitive.
Third, if you decide at any point that formal SEM training is not the right path, you have a full GP career to fall back on, or you can pursue the GP with special interest route (more on that below) without needing to retrain.
There are practical advantages too. You can locum as a GP alongside SEM training if finances are tight. GP locum rates are good. And getting medical indemnity as a qualified GP is typically more straightforward than with MRCP or MRCEM alone, which matters when you start doing clinical work outside your training programme.
The trade-off is the same three-year timeline as ACCS, and less acute or procedural experience compared to the ACCS route.
Which should you choose?
There is no wrong answer, but here is how I would frame it. If you want the fastest route and you are certain about SEM, Internal Medicine Training. If you want strong acute and procedural skills for pitchside or event medicine, ACCS. If you want maximum career flexibility and the safety net of a GP CCT, GP training. If you are not sure yet, GP training gives you the most options.
The GP route
Before SEM became a formal specialty, most sports doctors in the UK were GPs with a special interest. They completed GP training, developed expertise in MSK medicine and sports care through experience and additional qualifications, and built careers working with teams, clinics, and events. Some of the most experienced sports doctors in the country came through this route, simply because the formal SEM training pathway did not exist when they were training.
That route still exists today, and the Faculty has recently moved to formalise it.
GPwER in MSK Medicine
In 2026, FSEM launched the GP with Extended Role (GPwER) in Musculoskeletal Medicine accreditation. This is a structured, nationally recognised process for GPs who are already working in extended MSK roles to have their competencies formally assessed and accredited.
The accreditation is not a training programme. It is a portfolio-based assessment for GPs who are already doing the work and want formal recognition for it. You need to hold the FSEM Diploma in Musculoskeletal Medicine and be a Diplomate Member or Member of the Faculty in good standing to be eligible. The cost is £850 at the time of writing, and there are two application windows per year.
This gives GPs working in extended MSK roles a nationally recognised accreditation route. It does not make someone an SEM consultant, and it is not a substitute for SEM higher specialty training. For GPs who do not want to (or cannot) commit to four years of HST but want their MSK expertise recognised at a national level, this is the pathway. Full details are on the FSEM GPwER page.
How the GP route differs from consultant SEM
A GP with extended role in MSK medicine is not the same as an SEM consultant. The scope of practice, the clinical governance arrangements, and the professional standing are different. A CCT in SEM through formal training gives you consultant-level autonomy and recognition. The GPwER accreditation gives you formal validation of extended competence within a GP scope of practice. Both are legitimate careers. Which one suits you depends on how far you want to take the specialty and what other commitments you have.
FSEM diplomas and membership
The Faculty runs three diploma examinations, each focused on a different area of SEM practice:
- Diploma in Musculoskeletal Medicine (DipMSK): the MSK foundations exam, runs annually in May
- Diploma in Team Care (DipTC): focused on team and event medicine
- Diploma in Exercise Medicine (DipExMed): focused on exercise prescription and physical activity as treatment
Pass all three and you can apply for Membership of the Faculty (MFSEM), which at the time of writing will likely become MCSEM once the FSEM-BASEM merger into the College of Sport, Exercise and Musculoskeletal Medicine is complete. Holding all three diplomas demonstrates breadth of commitment and expertise across the specialty and is widely recognised within the SEM community.
It is worth being clear that the diplomas evidence knowledge and commitment. They do not, by themselves, make someone an SEM consultant or independently qualify them for all areas of SEM practice. They are one important component of a broader career in the specialty.
The diplomas are open to doctors, physiotherapists, and other eligible healthcare professionals. They are not restricted to SEM trainees. Many candidates sit them while in GP training, IMT, or ACCS to strengthen their ST3 applications, and many GPs use them as part of their extended-role development. I wrote about the DipMSK exam in detail in How I passed the FSEM Diploma in MSK Medicine.
The Portfolio Pathway (formerly CESR)
The Portfolio Pathway, formerly commonly referred to as CESR (Certificate of Eligibility for Specialist Registration), is the alternative route to the GMC Specialist Register for doctors who have not completed a GMC-approved SEM training programme but can demonstrate the required knowledge, skills, and experience to practise as a specialist.
In SEM, this means assembling a portfolio that proves you meet the same standards as someone who has completed ST3 to ST6. The evidence requirements are extensive: clinical logbooks, supervisor reports, audit projects, teaching evidence, examination passes, and structured references. The application is assessed by the GMC with specialty-specific evidence guidance, and if successful, leads to entry onto the Specialist Register. It does not award a CCT. The distinction matters: CCT is specifically for doctors who complete a GMC-approved training programme.
In practice, the Portfolio Pathway is significantly harder and more time-consuming than doing the formal training. It requires meticulous planning, years of documented experience, and a level of paperwork that most people underestimate. It is not a shortcut. Most people who can access formal training choose formal training.
That said, the Portfolio Pathway has been an important route for some of the earliest UK sports doctors. The ones who were working as GPs with special interest in sports medicine long before the formal pathway existed have now built decades of experience. For them, this route is the way to formalise what they have already been doing and gain specialist registration that reflects their actual competence.
If you are early in your career and have the option of applying for SEM ST3, I would take the formal training route. The Portfolio Pathway is best understood as a backup or a late-career formalisation, not a primary plan.
Where to start
If you are a medical student or foundation doctor and this specialty interests you, the single best thing you can do right now is visit the FSEM website and read through their careers and training pages. They are detailed and accurate.
Beyond that, start building exposure. Attend BASEM conferences. Provide medical cover at local sporting events. Get involved with your university or deanery sports medicine society if one exists. Find out who the SEM consultants and trainees are in your region and ask to shadow them. The ST3 application is competitive enough that the candidates who get offers are the ones who can demonstrate sustained interest and relevant experience, not just exam results.
I will be writing more on this. A future piece will cover practical tips for building a competitive SEM portfolio and strengthening your ST3 application. Another will cover routes into SEM for physiotherapists, nurses, paramedics, and other non-medical clinicians, because the specialty is genuinely multi-professional and the pathways for those groups deserve their own proper treatment.
For now, if you have questions about getting into SEM that this piece does not cover, you can reach me through the contact page. I read everything that comes in.